Life After Death
After a series of concussions left me with debilitating treatment-resistant depression, I finally found a treatment that worked — but I didn’t hear about it from a doctor. I heard about it from a friend.

Listen to this story:
My time of death: February 28, 2008, 8:02 p.m.
The low droning thrum of the Transcona industrial park reverberated through the frigid prairies, clinks and clangs echoing in the distance. Flurries drifted across the slick, pot-hole-infused roads like an army of ghosts fleeing Winnipeg’s arctic torture chamber. Patches of transparent ice glazed the pavement, forcing drivers to play a wicked game of ✨ Will I Die Today? ✨ In true Canadian fashion, some drivers treaded carefully, white-knuckling the steering wheel, while others blasted by like the laws of physics didn’t apply to them.
I was a white-knuckler. I gripped the steering wheel of my 1985 Oldsmobile Firenza as I drove home from the University of Winnipeg. Perhaps I was rehearsing a scene from the “ten-minute comedy duet” BARBIE AND KEN for my Intro: Performance class. Or perhaps I had gotten together with a few friends to sing songs from Urinetown: The Musical, our musical hyperfixation at the time. Maybe it was both. I don’t quite remember. What I do remember is, on that night, I made an impulsive decision that impacted the rest my life.
Approaching the stoplight at Plessis and Dugald Road, I peeked my head up like a wide-eyed gopher as I scanned for the lights of an oncoming train. Back then, there wasn’t an underpass. Trains came every few hours and would last anywhere from 15 minutes to an hour (if you were lucky). Going down Plessis was always a gamble.
Resting back into my seat, a seemingly brilliant idea surged through my mind: What if I went down Dugald instead? Still a possible train there, but a higher speed limit, so maybe I’ll get home faster.
Don’t do it, my instincts pleaded.
I did it anyway.
Even though the speed limit was higher, I still had to go 50 km/h — the same speed I would have gone down Plessis. The roads were too icy, too unpredictable to go any faster.
If only the driver’s ed instructor who slid into my lane at 70 km/h thought the same thing.
I remember looking down to change the radio station. When I looked back up, there was a car in front of me.
I’m going to die.
The impact was deafening — metal colliding, glass shattering, tires squealing — my neck snapping, my nose crunching, my teeth shattering against the steering wheel. My airbag-less car slid into a ditch; his car burst into flames. Blood gushed down my face as I clutched the steering wheel, fighting the pull to join the ghost army drifting across crushed stamped steel.

While my physical body remained alive, my bubbly personality, sense of self, and ability to feel joy died that night. The impact left me with a traumatic brain injury (TBI) that eventually turned into treatment-resistant depression — a form of major depressive disorder diagnosed after at least two different antidepressants aren’t enough to manage the condition during a depressive episode.
The depression got worse over time, and back then, I didn’t know why. According to a case report published in the Journal of Psychiatry Spectrum, an estimated 30 to 50 per cent of adults with moderate-to-severe TBI present with depression in the long term. First, it started with low moods and becoming “so negative,” or — as one of my past employers declared in front of all my co-workers — a “dark cloud.” Over the next 15 years, I went from being a “dark cloud” to spending hours — sometimes days — paralyzed in bed, as though a 10,000-pound boulder weighed me down. I’d cry so hard I’d choke on my own spit. I’d grasp my blue blankie, howling a stream of muffled I wanna dies until it was drenched with tears and phlegm, my throat raw.
On the rare days I was able to get out of bed, I’d sit in my car blowing my voice out as I howled the usual chorus of I wanna die, binding my scarf — sometimes my own hands — around my neck in hopes of escaping the hell I was trapped in.
Calling crisis lines became as common as ordering pizza.
I went to multiple doctors hoping to find some answers. They all told me to eat healthy and get more exercise while prescribing medication that made me panic, disassociate, and lose access to my memories.
I was a shell.
A husk.
A corpse.
Black ice, black veil
An osmium muzzle taut against my frame
Neural circuits short-circuiting
Somnia, hyper
Paralysis, laden
A frail yearning for revival
Just Think Positive!
I have spent 46.8 per cent of my life wanting to die.
A year after the car accident, I pursued a career in the performing arts, pushing through the mild depressive episodes I started to experience. I hustled hard — and I did get a lot of work — but I never got that big break. The constant rejections, toxic work environments, and financial instability inspired my internal monologue to go from you’re an unlovable failure to you should kill yourself.
In 2017, I moved to Toronto for more work opportunities, but by that point, I had hustled myself into burn out. I started having breakdowns, and I decided it was time to find another career. I ended up doing a lot of background and stand-in work so I could take some time to rest between shows and figure out what to do next. In 2019, I landed a seven-week gig on Work It, a Netflix comedy starring Sabrina Carpenter and Liza Koshy. I was Sabrina’s stand-in/photo double, and due to a shortage of five-foot-tall stand-ins, I didn’t have a backup if something happened.
On day nine out of 33, something did happen — my bicycle tire got caught in a streetcar track on my way home from set. Landing shoulder-first, my rose gold helmet smashed against the pavement as I slid across shards and pebbles. I was taken to the hospital and — unsurprisingly — diagnosed with a concussion. I went back to set the next day, pushing through the pain, fatigue, inflammation, nausea, dizziness, and brain fog, but I was sent home to rest for the long weekend. From the outside, it looked like I got plenty of rest, spending most of that time in bed. From the inside, I was trapped; paralyzed, tears dousing my pillow with my phone to my ear, compassionate crisis responders on the other end trying to resuscitate me.
The following Tuesday, I pulled myself up by my bootstraps and went back to set. For the next five weeks, I masked the depression and concussion symptoms the best I could, pushing through the 10 to 16-hour days, lengthy commutes, high-pressure environment, and physical demands, each day coming home to a crisis responder on the other end of the line.
One month later, I got another stand-in job. I still had concussion symptoms and I was still in a depressive episode, but being an artist living in Toronto, I needed the money. I wasn’t even on set for five minutes when I bashed my head on a big metal light, landing me in the hospital yet again.
That’s when the paralysis, breakdowns, and self-harm got even worse. I couldn’t stop crying. I couldn’t stop my hands from wrapping around my neck. I couldn’t stop striking myself across the face for being a stupid, overdramatic, unlovable piece of shit. Every day I struggled not to make my death permanent.
Desperate, I consulted Dr. Google and stumbled across a concussion clinic. A week later, I started treatment. The neurological physiotherapist told me I never properly healed from my car accident, so I was extra susceptible to head injuries. She used an eclectic mix of traditional and alternative therapy techniques like gua sha, dry brushing, stretching, deep breathing, castor oil, supplements, and anti-inflammatory diets. She also gave me an ear plug to put in my left ear — the side opposite of the impact — which instantly alleviated my grueling tension headache.
Over the next few weeks, I slept for 20-35 hours at a time. Slowly, I started to feel relief from my symptoms.
But even though I was healing from the concussions, I was still depressed.
What Do You Have to Be Depressed About?
After spending most of the pandemic isolated in my mouldy, mouse-infested apartment trying not to follow through on my ideation, I moved back home to Winnipeg. Despite being with family, things didn’t improve much. I no longer had a family doctor, so I went to the walk-in clinic down the street to see if there was anywhere in town that could help.
As the doctor typed up a referral for a neurologist, I expanded on my struggles and mentioned my hopes to find treatment options I hadn’t considered before.
She continued typing, her face stoic.
“Have you tried exercising?”
After seeing more than 20 medical professionals over the years about my treatment-resistant depression, I finally found a treatment that worked for me — but I didn’t hear about it from a doctor. I heard about it from a friend.
It was May 2023. I was lying in bed, unable to move, wanting to die. It was my birthday. I got a few happy birthday texts, including one from my friend Adrienne Sproule. As we were catching up, my thumbs moving so slow it put the Zootopia sloth to shame, she sent me the following text:
“Tms?” “Magnet therapy?” “Clear brain!?”
I minimized the Messages app and consulted my trusty ol’ pal Dr. Google.
I learned that TMS, also known as rTMS, stands for “repetitive Transcranial Magnetic Stimulation” and is a “noninvasive therapy that uses magnetic pulses to change brain activity.”
So, shock therapy? They still do that?
I kept reading:
“TMS works by using a small coil placed on your head. It sends magnetic pulses into your brain. These pulses pass through your skull and create tiny electrical signals in your nerve cells underneath. Depending on the pulse pattern, TMS can help wake up underactive areas or calm overactive areas.”
I still didn’t get it.
I remember going to YouTube to gain a better understanding, but I don’t remember what I watched. It may have been this “What is TMS?” walkthrough, or it may have been this “What Is TMS?” video:
Whatever it was, I remember getting only slightly more clarity on how the treatment worked.
I then went to Reddit to read about people’s personal experiences. Some people experienced 100 per cent remission. Others said it didn’t work for them, while one guy wrote an article about how it damaged his brain and created a Victims of Tms Action Group (VTAG), a Facebook group that, at the time, had over 4,000 members coming forward about how rTMS ruined their lives.
My brain was already damaged and my life was already in ruins, so I thought, fuck it. Might as well try it. What do I have to lose?
Driving up to the walk-in clinic, my heart was pounding, my stomach in knots. At the time, the St. Boniface Hospital’s rTMS program was the only place that offered the treatment free-of-charge, thanks to research funding, grants, private donations, and some government funding, according to Dr. Jitender Sareen, Department Head of Psychiatry at the University of Manitoba and Provincial Specialty Lead for Mental Health and Addictions at Shared Health. I didn’t have the money to pay for treatment at the private clinics, so it felt like everything was riding on this referral.
I remember the look on the doctor’s face when I uttered the words “TMS.” Her brow furrowed and eyes narrowed as she tilted her head slightly to the side.
“What is that?” She asked, wary, probably trying to decide if I was of sound mind.
I explained it the best I could, adding that I went to the neurologist and tried all the things a depressed person is supposed to do to feel better, according to medical professionals and the Dealing with Depression digest I impulsively bought in a checkout line hoping it had the elixir I so desperately needed. (It did not.)
When I mentioned the TMS program was at St. Boniface Hospital, the doctor shrugged, turning to her computer to write the referral. My shoulders fell away from my ears and the knots in my stomach untied.
I had my consultation in July, and in August, I started treatment.
Tick
tick
tick
tick
tick
tick
tick
tick
tick
tick
Low-lying clouds form, and part
The pogonip thaws, cross-dissolving to radiation—
A metamorphose in the beige barricades
The muzzle loosens
The tulle softens
slipping
surrendering
Between purgatories of then and now,
and sterile shades of sour milk
I remember seeing the rTMS machine for the first time. I thought it looked like something out of a sci-fi movie — an electric chair designed to shock me to death and turn my carcass into a Stormtrooper, programmed to defend the powers that be.
Thankfully, I did not turn into a Stormtrooper (that I know of), and it wasn’t nearly as scary as I thought it would be.
Ten minutes after my first session, I walked with my dad through La Vérendrye Park in a daze. Exhaustion is a common side effect of rTMS, especially during the first few days of treatment, so I was required to have a ride home.
As I fought to keep my eyes open and body upright, I stopped walking, my brow furrowing, eyes wide. Suddenly, the trees became greener, the sky bluer. I noticed the squirrels hopping through the grass and the monarchs gliding through the breeze. I felt the warmth of the sun soaking into my bones, my lips curling into a soft smile.
For the first time in 15 years, I felt a glimmer of joy for simply being alive.
I was not surprised when the psychiatrist deemed me a “responder.” While the dips I experienced during the transition phase were rough, my brain started to level out within about six months. I started socializing. I started laughing again. I was able to wash my dishes and take out the garbage. Over the next two years, my breakdowns became few and far between. My mom said I started physically carrying myself differently. I became “more talkative, more engaging.” I was functional, stable, content — all things that felt completely out of the realm of possibility a few years prior.
But, despite the welcomed metamorphosis, I couldn’t shake this one question: after seeing so many medical professionals about my incapacitating depression, why hadn’t any of them given me a referral for rTMS?
Ten years ago, I sat across from Adrienne in a converted pew booth, anxiously dipping a teabag in a mug of lukewarm water as she nursed a glass of beer. We were at The Toad in the Hole, an eccentric Winnipeg pub. It was my first date with a woman, and I remember starting to understand the jokes guys made about their nerves.
We met on Plenty of Fish, back when the site looked like a mix between Myspace and a semi-decent GeoCities site. The date went great, but after going out a few more times, we realized we fit better as friends. We became the kind of friends that may not talk or hang out for months at a time, but whenever we did, it felt like coming home.
I always felt a deep kinship with her. We both struggled with depression in similar ways: suicide ideation, continuous crying, oversensitivity to hormone fluctuations, difficulty concentrating, and wailing meek I wanna dies through harrowed sobs.
In 2017, Adrienne moved from Winnipeg to Vancouver, so I didn’t see her much anymore. But we kept in touch, keeping each other updated, supporting each other through our episodes, and wishing each other happy birthday.

Some People Have It Worse
Despite working as a nurse on and off for 10 years, the first time Adrienne heard about the treatment was when her psychiatrist casually mentioned it during a monthly follow-up. She was told that the University of British Columbia (UBC) was doing a study on rTMS and looking for participants. Meeting all the criteria, she got accepted into the study.
Adrienne was given the “real treatment” as opposed to the placebo. Within three days, she had energy for the first time in years. She was able to make appointments and go out for walks. Within a week, she started working out, going for hikes, and seeing friends — things that were next to impossible just seven days earlier. Like me, she was also a “responder.”
But rTMS is not a one-and-done treatment. It requires long-term maintenance, anywhere from months to years depending on the patient.
Think of rTMS like physical therapy for your brain. The first three weeks of treatment are like guided workouts that help “retrain” underactive brain circuits. Maintenance sessions are like going back to the trainer every few months to help those brain circuits stay active and functional.
After Adrienne’s initial one-week treatment, she started maintenance four months later. The UBC used a different machine on a different part of her head, and after that first round of maintenance, she never heard from them again. In rTMS Treatment for Depression: A Practical Guide by Paul B. Fitzgerald and Z. Jeff Daskalakis, it states, “As is the case with other antidepressant therapies, relapse rates appear to be relatively high in the period of time following the cessation of an acute course of rTMS treatment.” Over the next six months, this was exactly the case — all the positive effects wore off and Adrienne’s previous symptoms returned.
Have You Tried Yoga?
While rTMS is covered in Manitoba, it isn’t covered in British Columbia. According to the BrainWave Clinic, a neuropsychiatry clinic offering rTMS treatment in Winnipeg, a full course of rTMS could cost between $3,000 and $12,000 in clinics across Canada where it is not publicly covered.
Adrienne experienced the impacts of this hefty price tag when she tried to access further treatment. She’s been unable to work for four years due to her incapacitating depression and incessant suicide ideation, which makes affording an out-of-pocket expense like that impossible. It has been torturous for her to know there’s a treatment out there that works but is out of reach.
rTMS wasn’t always covered in Manitoba.
In fact — despite the first TMS device being invented in 1985 by Dr. Anthony Barker and his colleagues while futzing around with a Faraday coil on the brain’s motor cortex and being approved by Health Canada in 2002 — rTMS didn’t come to Manitoba until 2012.
According to Dr. Sareen, Dr. Mandana Modirrousta (owner-operator of the BrainWave Clinic) and Dr. Murray Enns founded the St. Boniface Hospital rTMS clinic in 2012 and conducted small research studies on Manitobans. From there, it took 11 years for the treatment to be covered under the provincial healthcare plan, which went into effect on October 1, 2023.
“Usually, a new discovery takes 30 years, and new treatments take about 15-20 years before health systems start to adopt it,” said Dr. Sareen in a virtual interview. “There has to be enough evidence for government to say ‘Yes, there’s enough evidence around this, and it’s cost-effective.'”
Once there was enough local evidence in the province to help build their case, Dr. Sareen worked alongside Dr. Modirrousta to create an Interventional Psychiatry Proposal for the Manitoba government, which helped get rTMS covered under the provincial healthcare plan and incorporated into Manitoba’s model of care.
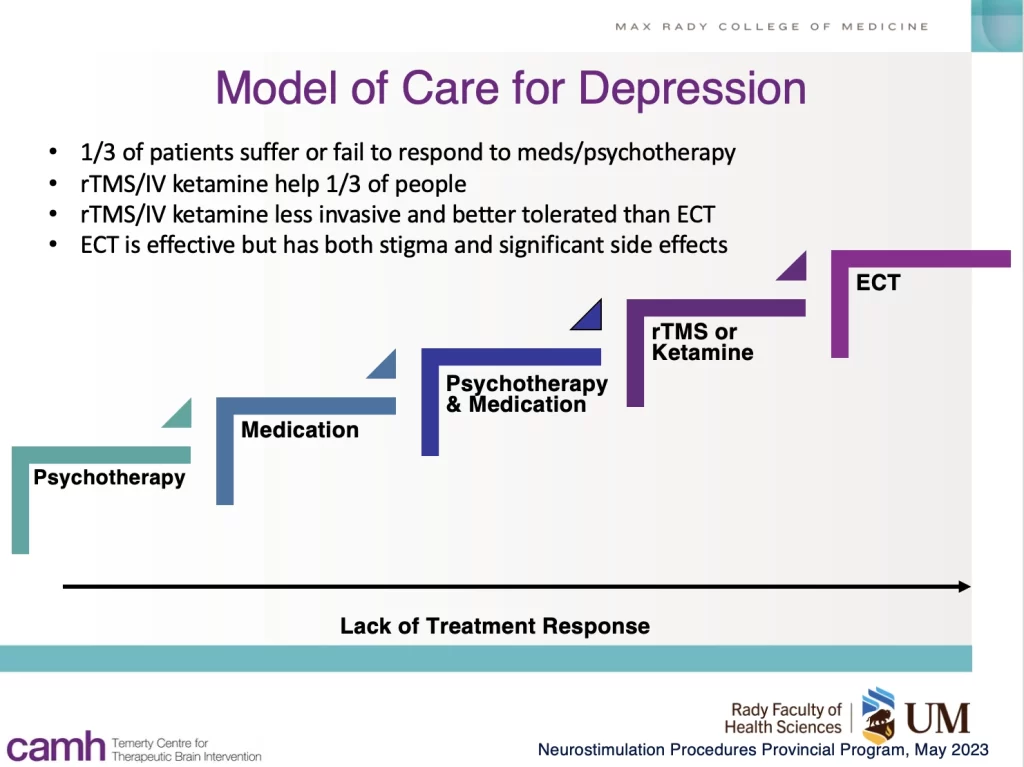
Before the incorporation, treatment for depression would start with psychotherapy. If that didn’t work, the patient would be put on medication, and if there still was no improvement, the patient would move to a combination of psychotherapy and medication. From there, the next step was electroconvulsive therapy (ECT) — an effective but intense treatment with significant side-effects and stigma that requires general anesthesia while inducing a brief, controlled seizure. rTMS and IV ketamine now bridges that gap between psychotherapy plus medication and ECT.
As I looked through the proposal Dr. Sareen shared with me, one line slowed time itself, bringing me to a standstill: “rTMS has evidence in other conditions such as concussion.”
Holy shit. rTMS was the elixir I needed all along.
After talking to Dr. Sareen, I started to understand why I never received a referral for rTMS without asking for one—at least in Manitoba.
Even though the treatment has been around since the 1980s, has lots of international evidence-based research, and was added to the depression guidelines taught in medical schools in 2016, rTMS was only recently added to Manitoba’s model of care due to the need for more local evidence, funding, and infrastructure within the province.
And according to Dr. Sareen, medical students get lectures on depression, which covers rTMS. However, they’ll only have the chance to learn more about it if they have a psychiatry clerkship at St. Boniface Hospital, or if they have a psychiatry residency. Otherwise, they have to take an elective.
Dr. Sareen is currently working with regions throughout Manitoba to create a centralized referral system, which includes a website dedicated to providing accessible information to Manitobans.
With Québec, Saskatchewan, Yukon, Alberta, and Manitoba now covering the treatment through provincial healthcare plans, I have two hopes: one, that physicians begin referring patients for rTMS when recommended; and two, that health coverage spans the country so people like Adrienne can access the care they need.
Tick
tick
tick
tick
tick
tick
tick
tick
tick
tick
Thawed ice, thin veil
A fascinator fastened upon strawberry locks,
for teatime with The Reaper
and a welcomed farewell
Neural circuits surging,
dark clouds dispersing,
sparking the dawn of a hereafter
Snapping Out of It
At the time of writing this, I’d consider myself close to remission. I’ve been able to go back to school and lead the Rainbow Resource Centre’s Bi+ Social Group. I’ve been able to make conversation with strangers, regulate my emotions, and generally function the way people are supposed to. I’ve even been able to follow doctor’s orders and get more exercise! I still have depressive episodes, but rather than lasting weeks, they last hours — sometimes minutes. And instead of wanting to die, I mostly just want to sleep.
This even applies when I get concussions. Being the silly goose I am, I’ve bonked my head a few times since starting treatment. While I had short-term brain fog, dizziness, and fatigue, I didn’t get depressed.
rTMS doesn’t work for everyone, but it resuscitated me — the copper coils and magnetic pulses bringing me back to life after what felt like my death.
The dark clouds gone, I face the sun, basking in the joy of simply being alive.
Podcast recording voiced by ACTRA member Amanda Haley (Mandi) Maxwell. Visit her website to book her for performance work.